


 i_need_contribute
i_need_contribute
Part 1: The Widespread Use of CAM and the Need for Better-Informed Health Care Professionals to Provide Patient Counseling C. Lee Ventola, MS
This is the first in a series of three articles on the use of complementary and alternative medicine (CAM) and dietary supplements. Part 2 will discuss regulation, drug interactions, and other safety issues, as well as sources of information about dietary supplements. The third article in this series will focus on the policies and practices regarding CAM and integrative medicine in health care facilities.
Introduction
Nearly 40% of adults in the U.S. use some form of complementary and alternative medicine (CAM) therapy, including dietary supplements.1,2 The widespread popularity of CAM and dietary supplements has brought attention to the existence of both a knowledge and a communication gap for health care professionals with respect to being able to properly counsel patients about these treatments.3–8 A lack of evidence-based information about efficacy, safety, and drug interactions with CAM therapies, as well as a lack of formal training, is thought to be responsible for this deficit.3–6,8 Although the federal government, academia, and the private sector have begun to offer some support for CAM education, research, and integration with conventional medicine, more initiatives are needed.5,9–13 Professional standards regarding CAM that have been issued for pharmacists and physicians are an important source of guidance in providing patient counseling and utilizing these treatments.4,5,14–16
What Is CAM?
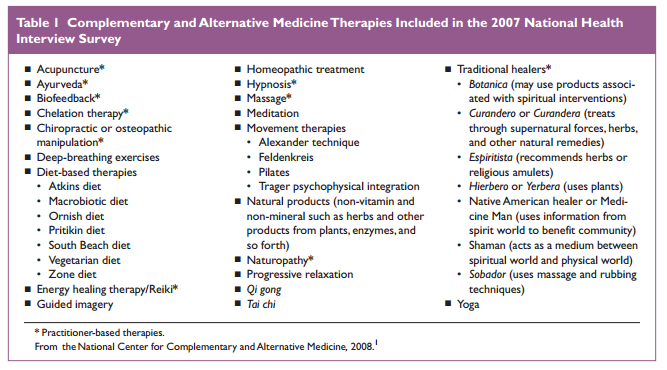
The National Institutes of Health (NIH) has defined CAM as “a group of diverse medical and health care systems, practices, and products that are not presently considered to be part of conventional medicine.”1,4 The National Center for Complementary and Alternative Medicine (NCCAM) further classifies CAM therapies into five distinct categories:1,8,9
• alternative whole medical systems (homeopathic and naturopathic, Chinese, and Ayurvedic medicine)
• mind–body interventions (meditation, prayer, mental healing, art, music, and dance therapy)
• biologically based therapies (herbs, foods, vitamins and other dietary supplements, including natural products such as shark cartilage)
• manipulative and body-based methods (chiropractic and osteopathic manipulation, massage)
• energy therapies (qi gong, Reiki, therapeutic touch, and electromagnetic field exposure).
Dietary supplements, or nutraceuticals, fall into the subcategory of CAM called “biologically based therapies.”1,8,9 The quantity and diversity of these products are enormous.8 Supplements include herbs, minerals, teas, vitamins, amino acids, animal tissue extracts, essential oils, and Asian medicines taken orally for the purpose of promoting health and nutrition.8,17 In the U.S., dietary supplements are considered to be “functional foods,” used for health benefits other than nutrition, and they are therefore regulated as foods instead of drugs.8 As for the difference between “complementary” and “alternative” medicine, the former is used together with conventional medicine, whereas the latter is used in place of it.15 “Integrative medicine” refers to a therapeutic approach that integrates conventional, complementary, and alternative medicine and re-emphasizes the relationship between health care practitioners and patients.1,5
History of CAM in the United States
In American history, the distinction between conventional medicine and CAM began in the early to mid-19th century.12 During this time, alternative medical practitioners gained popularity and began to compete with conventional medical professionals.12 Alternative practitioners based their practice on theories of health and healing that were intentionally different from those in conventional medicine, emphasizing “safe” or “natural” therapies and the emotional and spiritual aspects of health.12 Many patients found this approach appealing, resulting in the promotion of competition between alternative and conventional medical practitioners throughout the 19th century.12 However, in the early to mid-20th century, evidence-based medicine became increasingly important, as scientific experimentation led to discoveries about the human body, diseases and treatments, diagnostic techniques, and vaccines, all of which caused the popularity of alternative medicine to wane.12 Although practitioners of orthodox medicine have historically often vigorously denounced and attacked alternative practices, some of these methods have been adopted as conventional treatment regimens.11 The only effective malaria treatment for more than 300 years—quinine—is an important conventional drug that was derived from an unconventional therapy (Cinchona or Peruvian bark).8 The clinical use of foxglove in ancient times led to the modern-day use of the cardioactive drug digoxin, morphine and codeine were originallyderived from the poppy plant Papaver somniferum, and salicylate was originally isolated from willow tree bark.8 In fact, 25% of modern pharmaceutical products were originally derived from plants, and it is estimated that as many as 70,000 plants have been used as medicine throughout history.8
Use of CAM and Dietary Supplements Is Widespread
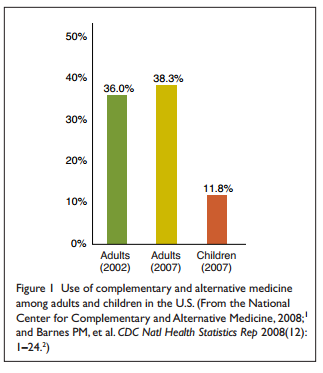
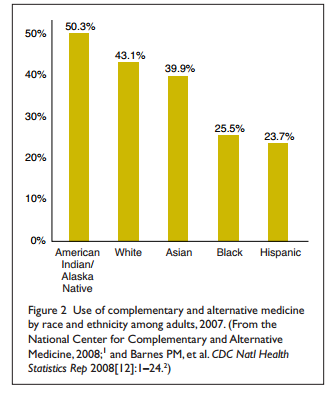
Survey Results Although the popularity of CAM waned in the early 20th century, it has since rebounded. In December 2008, the NCCAM and the National Center for Health Statistics (NCHS) released the latest findings on Americans’ use of CAM.1,2 These results were from the 2007 National Health Interview Survey (NHIS), which collected information for 23,393 adults and 9,417 children under the age of 18.1,2 The data showed that 38% of adults and 12% of children in the U.S. were using some form of CAM (Figure 1 and Table 1).1,2 These results represented an increase in use from 2002, when 36% of adults had been found to be using CAM (see Figure 1).1,2 CAM usage was observed among people of all backgrounds; however, its use was more frequent among women and adults with higher incomes and advanced levels of education.1,2,11 Usage of CAM was also substantial across all ethnic groups but was more common among Native Americans and less common among African-Americans and Hispanic-Americans (Figure 2).1,2,11
• had parents who used CAM (23.9%).
• were adolescents 12 to 17 years of age (16.4%).
• were Caucasian (12.8%) rather than Hispanic (7.9%) or African-American (5.9%).
• had parents with higher education levels (14.7%).
• had six or more health conditions (23.8%).
• experienced delayed conventional care because of cost (16.9%).
Use of CAM Among Children
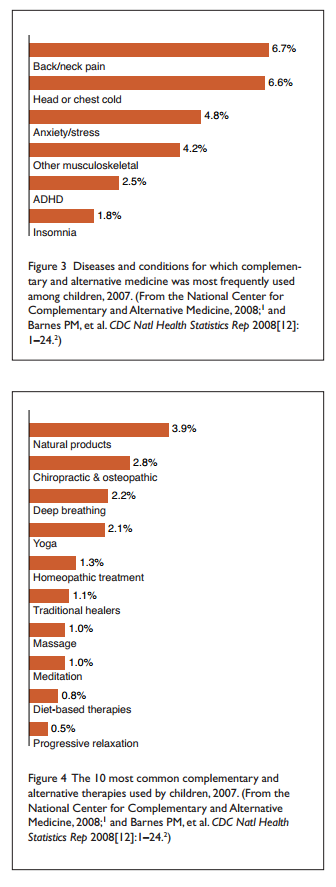
The use of CAM and dietary supplements was found to be fairly common in children and adolescents, especially those needing frequent medical care and hospitalizations for chronic conditions.1,6 According to adult respondents who were asked about use by non-adults in their household, the use of alternative therapies was greater among children who:1,2 Survey findings on the pediatric use of CAM and dietary supplements, with respect to diseases or conditions and top therapies, are shown in Figures 3 and 4.1,2
Dietary Supplements Are the Most Frequently Used CAM Therapy
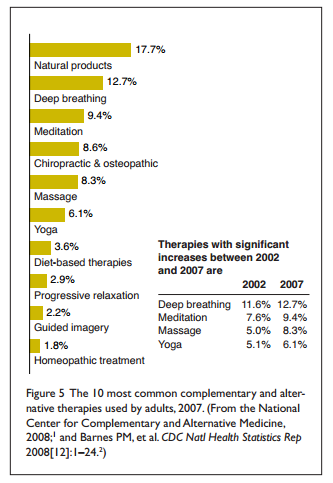
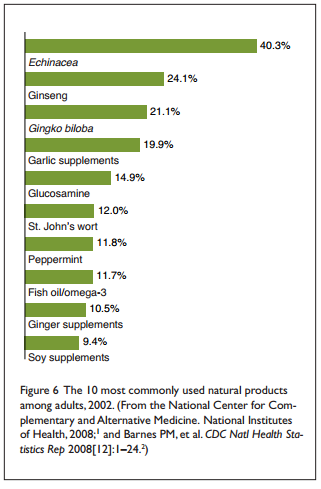
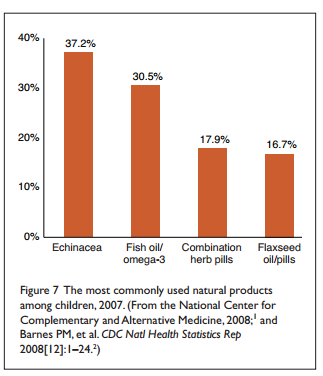
“Natural products” (i.e., non-vitamin, non-mineral supplements) were the most commonly used CAM therapy for both children and adults (Figures 4 and 5).1,2 Echinacea and fish, omega-3, and flaxseed oils were among the most popular natural products used by both age groups (Figures 6 and 7).1,2 Other popular therapies included deep-breathing exercises, meditation, massage therapy, and yoga.1,2
Health Conditions Prompting CAM Use
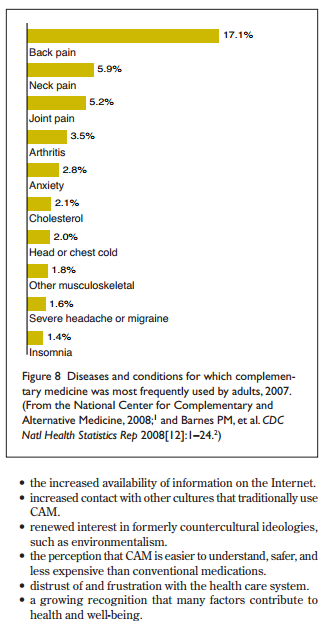
Although CAM has been used to treat a variety of diseases and conditions, the NHIS and many other studies have found that CAM usage occurs most frequently among people with poorer health status resulting from chronic, recurrent, or seri ous ill ness (Figures 3 and 8).1,9,11,17 For example, CAM use has been noted to be prevalent among patients with allergies, asthma, behavioral and developmental problems, cystic fibrosis, HIV infection, rheumatoid arthritis, and musculoskeletal problems such as back, neck, or joint pain.1,17 Two-thirds of chronically ill patients have used dietary supplements, frequently concomitantly with prescription and over-the-counter drugs.17 According to the National Cancer Institute, part of the - National Institutes of Health, the use of CAM is even more prevalent among cancer patients.11 In one study, 83% of 453 cancer patients were reported to have used at least one CAM therapy as part of their treatment regimen.11 In another study, more than 50% of cancer patients were using CAM therapies with, prior to, or following conventional therapies.11 These findings are concerning because patients who are already receiving complicated conventional treatment regimens are at a greater risk for adverse events, especially because many supplements have not been evaluated for safety, efficacy, or drug interactions.11,18
Expenditures for CAM Therapies Continue to Grow
The amount of money spent on CAM treatments in the U.S. has skyrocketed in recent years.18 According to the results of the 2007 survey, Americans spent $33.9 billion out of pocket on CAM therapies that year.18 About $22 billion was spent on natural products, instructional classes, and materials.18 Dietary supplements accounted for $14.8 billion of this amount, an expenditure equal to about one-third of out-of-pocket spending for prescription drugs.18 The remaining $11.9 billion was spent on an estimated 354 million visits to CAM practitioners (such as acupuncturists, massage therapists, or chiropractors), an amount equal to about 25% of out-of-pocket costs for visits to conventional doctors.18
Reasons for the Increased Use of CAM and Dietary Supplements
People use CAM for a variety of reasons.5,12 Patients have become more interested and informed about CAM because of: Increased public access to information and savvy consumerism have also led to a decreased tolerance of what patients may perceive as paternalism in the traditional practice of medicine.11 Patients may see conventional doctors as being overly reliant on prescribing drugs and as not bothering to explain the methodology, risks, and benefits of these treatments.12 Patients may be dissatisfied with conventional treatments because of adverse effects, cost, lack of efficacy, erosion of doctor–patient relationships, or an impersonal health care system.11,12,14 Media attention on the adverse effects and escalating costs of conventional medicines have also caused patients to look for alternatives for preventing and managing illness.11 Patients who are not satisfied with conventional medicine may also enjoy autonomy in making health care decisions and the resulting impression of personal control.10,17 They may prefer alternative therapies, which may be perceived as more per sonally empowering and less secretive and authoritarian.11 Paradoxically, the increased use of CAM might have also stemmed from the successes of conventional medicine.12 As advances in conventional medicine and public health led to a dramatic decrease in the number of deaths resulting from acute infectious diseases, the prevalence of chronic, incurable conditions increased.12 Patients expect conventional medicine to solve all health problems and tend to turn to or include alternative medicine treatments when traditional care fails.9,12 Patients with chronic conditions are also often attracted to the emphasis on health promotion and self-healing that CAM therapies provide.12 Cultural influences may also attract patients to alternative therapies that might be more compatible and consistent with their spiritual beliefs or world view.11 American society is multicultural and includes a large number of first-generation immigrants who routinely use or might have already explored CAM.9 Immigrants to the U.S. may also prefer CAM practitioners for a variety of reasons, such as favorable payment terms, use of methods that are familiar and have been used for generations, a common language, and other cultural factors.11 Public perception of CAM therapies as an attractive alternative to conventional medicine may also be enhanced by sophisticated marketing and promotion by the supplement industry.17 Supplements are sometimes sold alongside prescription and nonprescription medications, creating the impression that their potency, efficacy, and safety are equivalent to those of pharmaceuticals.17 Even though manufacturers are forbidden to make such statements, consumers are also exposed to discussions of disease-specific indications for dietary supplements in the lay media (e.g., glucosamine for osteo - arthritis, black cohosh for menopausal symptoms, and St. John’s wort for depression).17
Knowledge and Communication Gaps Prevent Proper Counseling of Patients
Studies have shown that most dietary supplements sold in the U.S. are purchased in pharmacies. Pharmacists, therefore, are in an especially good position to provide patients with information about the safety, efficacy, and potential drug inter - actions for supplements at the point of purchase.4 Pharmacists are also best able to document supplement use in the patient’s medical history and to determine the effect of alternative medications on the patient’s regimen of conventional medicines.11 Pharmacists also have the knowledge and experience to help patients determine whether self-medication is appropriate or whether they should see a health care practitioner instead.4 Because of fear of disapproval, patients may also feel more comfortable telling their pharmacist, rather than their physician, that they are using a dietary supplement in addition to prescribed therapies.11 Although pharmacists are in an ideal position to provide counseling and record-keeping, research suggests that few pharmacists or other health care professionals routinely ask about, document, or monitor patients’ use of dietary supplements.4–6 Pharmacists are uncomfortable answering questions about supplements because few scientific studies are available to guide clinical discussions and decisions, and they often do not feel knowledgeable about this topic.4–6 Pharmacistsmight also not be familiar with professional practice standards that recommend routine inquiry, documentation, and monitoring of patients’ use of supplements.4 Pharmacists who are most likely to inquire about and record supplement use work in inpatient settings, have access to evidence-based information on CAM, or have received additional training in alternative medications.4,5 Physicians also believe that they lack the resources and training to respond to patients’ inquiries about dietary supplements.3,8 In a recent survey in which more than 80% of the 164 respondents were general practice physicians (the remainder were mostly pharmacists), 76% said that they were “poorly informed” about herbal medicines and 46.6% said that their own knowledge on this topic was “very poor” or “quite poor.”7 Although 77.3% of respondents said that they feared their patients would take herbal medicines without telling them, only 12.9% said that they “always” inquire about the use of dietary supplements.7 In another study, more pharmacists than physicians rated their knowledge about CAM products as either “above average” or “excellent” and indicated that they could be a good alternative or adjunctive therapy to prescription medications, whereas physicians tended to state that they were either ineffective or unsafe.3 This difference was attributed to the pharmacists’ greater familiarity and interest in dietary supplements, as well as their having more experience counseling patients on this subject.3 In many health care facilities nationwide, a physician’s order is often required to allow patients to use a home supply of dietary supplements.6 These survey findings prompt the question about whether physicians have the training and confidence to issue such an order.6 Physicians should therefore be encouraged to utilize pharmacy services before ordering that a patient be permitted to take a supplement.11 Patients also contribute to the communication gap with health professionals.11 In one survey, 72% of respondents did not report their use of alternative therapies to their health care providers.14 Another study showed that although twothirds of chronically ill patients used dietary supplements, only 30% discussed their use with their physicians.17 This is a dangerous oversight, because many chronically ill patients also take prescription medications, putting them at a greater risk for supplement–drug interactions.5,18 In a study of Hispanic women, 40% of the subjects indicated that they never voluntarily reported CAM use to their physicians, and more than 60% replied that their physicians had never asked.11 Patients reported that they were reluctant to discuss the topic because they perceived a sense of disapproval by the physician with regard to CAM use.11 Patients’ reluctance to communicate about supplement use with doctors and pharmacists is just as significant a problem as health professionals’ hesitancy to discuss this topic with their patients.11 Pharmacists and other health care practitioners clearly have the opportunity to reduce medical risks by increasing their knowledge and communication about dietary supplements.14 The American Society of Health-System Pharmacists (ASHP) agrees that pharmacists, as medication-use experts and accessible health care professionals, are uniquely qualified and positioned to identify potential adverse drug events and interactions and counsel patients on using supplements.14 However, despite this professional responsibility, pharmacists and other health care providers are frustrated by the lack of sound, evidence-based professional resources for reliable information about the safety and efficacy of supplements.14 This situation is in contrast to the wealth of available evidence about most pharmaceutical treatments.14 Medical professionals are largely on their own when trying to understand the ingredients, proper indications, and dosages for the appropriate clinical use of supplements.10
Need for Education Regarding CAM Therapies and Dietary Supplements
In recognition of the widespread popularity of CAM, leading academic institutions are increasingly incorporating CAM into medical education, clinical practice, and research.9,10 A national Consortium of Academic Medical Centers for Integrative Medicine has been formed, composed of 42 academic centers whose goal is to advocate and foster research on CAM and integrative medicine.10 With support from the federal government, medical and nursing schools are incorporating lessons about CAM and dietary supplements into the education and training of physicians and nurses.5,11–13 For example, the University of Arizona Center for Integrative Medicine has medical residency programs in hospitals nationwide.13 The University of Minnesota also offers an elective course in alternative healing methods at a Hawaiian medical center.13 Although Harvard University does not claim to advocate or teach alternative medicine, students there are offered electives in mind –body medicine.13 Many pharmacists would also like to receive additional training in dietary supplements, especially in the areas of inter - actions, adverse events, patient counseling, therapeutic uses, and dosing.4 The ASHP supports the inclusion of course requirements on the taxonomy, formulation, pharmacology, and pharmacokinetics of supplements in pharmacy curricula.14 However, regardless of such interest and support, the extent of education on supplements offered by pharmacy schools is very inconsistent.4 Courses on CAM and dietary supplements aren’t usually incorporated into American pharmacy school curriculum requirements; if available at all, they are offered as an elective.4 However, the National Association of Boards of Pharmacy now includes questions about CAM and supplements on the North American Pharmacist Licensure Examination, which may be an impetus to make courses on these topics a requirement in pharmacy school curricula.5 Government and the private sector have also been influenced by popular trends regarding CAM.10 The federal government has already disbursed more than $22 million to support the inclusion of courses on CAM in medical and nursingschool curricula so that health professionals can competently discuss CAM with patients.13 However, much work remains to be done in this area with respect to faculty and curriculum development.10 Further support from the federal and state governments may be necessary to provide medical, pharmacy, and nursing schools the needed resources and incentives to make progress.10 In the private sector, some insurers have begun to cover CAM services and include alternative practitioners in their networks.10 Health care systems have also shown some interest in developing appropriate in-service training and continuing medical education (CME) programs on integrative medicine for health professionals.10
Professional Standards for Pharmacists and Physicians
Clear professional standards may provide health professionals with needed guidance when providing patient counseling on CAM and dietary supplements.4 Professional organizations such as the American College of Clinical Pharmacy (ACCP), the ASHP, and the Federation of State Medical Boards (FSMB) in the U.S. have issued such professional standards.4,14–16
Professional Standards for Pharmacists
The ACCP and ASHP recognize that pharmacists have an opportunity to develop a unique and credible professional role for themselves as expert advisers on dietary supplements; these organizations have therefore recommended that pharmacists actively embrace supplements in their scope of practice.4,14,16 In a white paper on herbal products issued by the ACCP, the authors argued that pharmacist expertise in herbal products is an “extension of their roles in pharmaceutical care, clinical pharmacy practices, and collaborative health care teams.”16 The report also suggests that “the variability in the degree of scientific evidence on efficacy and safety available to support the use of herbal products makes it even more imperative that pharmacists assume an active role in this area of practice.”16 The ASHP has similarly stated that “the widespread, in- discriminate use of dietary supplements presents substantial risks to public health and ... pharmacists have an opportunity and a professional responsibility to reduce those risks.”14 The ASHP “urges pharmacists and other health care practitioners to integrate awareness of dietary supplement use into everyday practice and encourages pharmacists to increase efforts to prevent interactions between dietary supplements and drugs.”14 The ASHP recommends that, at a minimum, pharmacists become familiar with the pharmacology and pharmaco kinetics of common supplements that might contraindicate concurrent use with prescription and nonprescription medications.14 In order to provide informed guidance to patients using or considering the use of dietary supplements, the ASHP advises that pharmacists should become knowledgeable about:14
• typical uses for common supplements as well as the scientific literature describing their efficacy and safety.
• proven and potential interactions between common supplements and conventional medications (both prescription and nonprescription).
• methods to therapeutically monitor the effects of common supplements, including signs and symptoms of potential adverse events and toxicities.
• proven and potential effects of certain disease states on the absorption, distribution, and elimination of dietary supplements.
• the safety of dietary supplement usage before or after surgery.
The ASHP professional guidelines also suggest that pharmacists and other health care practitioners routinely inquire about a patient’s current or planned use of dietary supplements, providing examples to ensure that the patient understands the questions.14 Obtaining accurate information from patients allows health care practitioners to provide counseling about and monitor for adverse reactions and drug interactions with supplement use.14 The ASHP also advises that during counseling about supplements, patients should be warned of the concept of caveat emptor (buyer beware) because the efficacy and safety of these products are not well regulated.14 Patients who are stabilized on a supplement and a medication should be cautioned not to suddenly discontinue the use of either product without first consulting the prescribing physician.14 Potential adverse effects from drug interactions may occur when the supplement is discontinued as well as when it is initiated.14 The ASHP also states that pharmacists have a responsibility to continually monitor the scientific literature in order to incorporate knowledge about dietary supplements into caring for and advising patients.14 Despite shortcomings in the data on these products, the limited references that are available should be consulted.14 Pharmacists should also review promotional and reference materials in the workplace to ensure that these materials are evidence-based and not deceptive or misleading.14
Professional Standards for Physicians
The FSMB has also responded to the increased interest in CAM by issuing its own guidelines.5,15 The board recognizes that consistency in standards for evaluating health care practices is necessary, whether they are applied to conventional medicine or to CAM.5,15 These guidelines provide a methodology by which to evaluate physician adherence to a state’s Medical Practice Act, as well as to “do no harm” criteria with respect to CAM and seven aspects of patient care: evaluation of the patient; preparation of the treatment plan; responsibilities during consultation or referral to other licensed health care providers; documentation of medical records; documentation of medical knowledge with respect to methods offered; requirements for the sale of goods from physician offices; and requirements for performing clinical investigations.5,15
The FSMB guidelines also urge physicians to first consider whether an alternative treatment is:5,15
• effective and safe, meaning that adequate scientific evidence exists for the efficacy and/or safety of a treatment (or, at least, greater safety than other established treatment models for the same condition).
• effective, but with some actual or potential danger (i.e., there is evidence of both efficacy and side effects).
• inadequately studied but safe (i.e., there is insufficient evidence of clinical efficacy but reasonable evidence to suggest relative safety).
• ineffective and dangerous (i.e., the treatment has proved to be ineffective and unsafe through documented evidence, controlled trials, or as determined by a risk–benefit assessment).
Conclusion
Studies show that pharmacists and physicians currently lack the knowledge, confidence, and training to provide proper guidance to the increasing number of patients who are using CAM therapies.3–8 Although the federal government, academia,and the private sector have begun to offer more support for education, research, and the integration of CAM with conventional medicine, more initiatives are needed.5,9–13 In the meantime, professional standards regarding CAM that have been issued for pharmacists and physicians are an important source of guidance with respect to providing patient counseling and utilizing these treatments.4,5,14–16
References
1. National Center for Complementary and Alternative Medicine (NCCAM). The Use of Complementary and Alternative Medicine in the United States. Bethesda, Md.: National Institutes of Health; December 2008. Available at: http://nccam.nih.gov/news/ camstats/2007/camsurvey_fs1.htm. Accessed June 15, 2010. 2. Barnes PM, Bloom B, Nahin R. Complementary and alternative medicine use among adults and children: United States, 2007. CDC Natl Health Statistics Rep 2008(12):1–24. 3. Dunn JD, Cannon HE, Lewis T, Shane-McWorter L. Development of a complementary and alternative medicine (CAM) pharmacy and therapeutics (P&T) subcommittee and CAM guide for providers. J Manag Care Pharm 2005;11(3):252–258. 4. Kwan D, Hirschkorn K, Boon H. U.S. and Canadian pharmacists’ attitudes, knowledge, and professional practice behaviors toward dietary supplements: A systematic review. BMC Complement Altern Med 2006;6(31):1–10. 5. McHughes M, Timmerman B. A review of the use of CAM therapy and the sources of accurate and reliable information. J Manag Care Pharm 2005;11(8):695–703. 6. Gardiner P, Phillip RS, Kemper K, et al. Dietary supplements: Inpatient policies in U.S. children’s hospitals. Pediatrics 2008; 121(4):e775–e781. 7. Most doctors not knowledgeable about herbals. HealthDay News, April 26, 2010. Available at: www.modernmedicine.com/modern medicine/Modern+Medicine+Now/Most-Doctors-Not-Knowl edgeable-About-Herbals/ArticleNewsFeed/Article/detail/666928. Accessed June 15, 2010. 8. Waldman SA, Terzic A. Pharmacology and Therapeutics: Principles to Practice. Philadelphia: Elsevier/W. B. Saunders; 2008:1536. 9. Vohra S, Feldman K, Johnston B, et al. Integrating complementary and alternative medicine into academic medical centers: Experience and perceptions of nine leading centers in North America. BMC Health Serv Res 2005;5(78):1–7. 10. Micozzi, MS. Integrative medicine in pharmacy and therapeutics. P&T 2003;28(10):666–672. 11. Cohen KR, Cerone P, Ruggiero R. Complementary/alternative medicine use: Responsibilities and implications for pharmacy services. P&T 2002;27(9):440–446. 12. Kantor M. The role of rigorous scientific evaluation in the use and practice of complementary and alternative medicine. J Am Coll Radiol 2009;6(4):254–262. 13. Demand fuels alternative medicine classes. CBS News, November 2, 2009. Available at: www.cbsnews.com/ stories/ 2009/ 11/ 02/ health/ main5498107.shtml. Accessed June 15, 2010. 14. American Society of Health-System Pharmacists. ASHP statement on the use of dietary supplements. Am J Health Syst Pharm 2004;61:1707–1711. 15. Federation of State Medical Boards (FSMB). Model Guidelines for the Use of Complementary and Alternative Medicine in Medical Practice. April 2002. Available at: www.fsmb.org/ pdf/ 2002_ grpol_Complementary_Alternative_Therapies.pdf. Accessed June 15, 2010. 16. Miller LG, Hume A, Harris IM, et al. ACC white paper: White paper on herbal products. Pharmacotherapy 2000;20(7):877–891. 17. Boyer EW. Issues in the management of dietary supplement use among hospitalized patients. Int J Med Toxicol 2005;1(1):30–34. 18. Alternative medicine spending soars. The Washington Post, July 30, 2009. Available at: http://voices.washingtonpost. com/ checkup/ 2009/07/alternative_medicine_spending.html. Accessed June 15, 2010. ■





 Research
Research
